We were at the Patient Academy in Bad Salzschlirf. Berthold Wilden (1st chairman of the MFSH) explained the topic of the “controversial” variants well and we then presented our statement from the patient’s point of view. Our statement is linked here.
In general, this topic was a big topic of conversation among the patients during the break, no one can understand the attitude and actions of the doctors. Now, however, many know about the topic and have backed us with a lot of encouragement that we should absolutely continue to fight. Many thanks for that.
It was also very nice for us to see many familiar faces again, we were very pleased.
An artist friend of ours provided us with a great picture that illustrates our theme very well:
image: Ralph Turnheim, www.leinwandlyrik.de
Image text: we do not extinguish further until the cause of the fire has been completely clarified
Part 2 explains basics of cell biology and genetics so you can understand Fabry in the first place. Part 3 then goes into the necessary details regarding Fabry.
A new website for Fabry patients and interested parties is online. There Fabry is explained in video in the simplest possible words. How does the disease etc. is explained in short videos piece by piece, the first videos are available, more will follow very soon.
Wir veröffentlichen hier Text und Link eines befreundeten Künstlers, der für eine Patientin kämpft und ihr (auch in unserem Sinne) mit allen Mitteln helfen will:
Eine enge Freundin von mir leidet an einer schlimmen, seltenen Erbkrankheit. Vor zwei Wochen hat ihr die Ärztin mitgeteilt, ihr das lebensnotwendige Medikament nicht mehr zu verschreiben. Die Geschichte ist so herzzerreißend wie absurd. In einem Podcast gehen wir dieser Geschichte nach. Hier ist die erste Folge – solange Carmen kann (sie hat noch eine letzte “Ladung” Medikamente bekommen, dann ist Schluss), wollen wir jede Woche eine weitere machen. Gebt mir gerne Feedback bzw. eure Fragen – wir gehen gern darauf ein. Sie freut sich über die Aufmerksamkeit, denn es sind viele andere betroffen. Danke!
Natascha and Berthold from MFSH were at FIN meetings in Amsterdam. FIN=Fabry International Network, an association of Fabry self-help groups from all over the world.
The presentation of the research work on “controversial variants” or D313Y was the highlight. The work could be presented to patients and scientists from all over the world.
Yes, at least in a certain proportion of patients.
There is always talk of an enzyme deficiency that leads to deposits in the cells and then triggers the malfunctions. In many missense variants (i.e. an amino acid is altered somewhere in the DNA on the GLA gene) there is a residual activity of the enzyme. Nevertheless, the patients are often also severely affected. Here, another mechanism comes into play: ER stress or Unfolded Protein Response (UPR).
A brief explanation: Due to the variant, the enzyme is formed, but it is partly defective. Now a kind of “quality assurance” kicks in in the cell. The faulty enzyme is “repaired”. This is a normal process in the cells, since minor errors can happen again and again. However, due to the variant, the enzyme is permanently formed incorrectly and the error correction is overloaded. This is ER stress, which can lead to malfunctions of a cell or even cause cell death. Caperone therapy also “repairs” the wrong enzyme and relieves the cell. Here, enzyme replacement therapy would be less effective.
This mechanism has been demonstrated for some time, including for some of the controversial variants. But this explanation is not accepted by all scientists because it contradicts their own publications.
We patients are the ones who suffer; we are then prescribed no therapy or a less effective one.
In Fabry and many other diseases, a genetic test is used to determine whether there are changes in the DNA (genetic material) that can cause a disease.
For some time now, “next generation sequencing” has been available for this purpose, i.e. the actual sequence of information on a gene is determined. In the past, this was not possible and special tests were developed that were applied to very specific gene sections (e.g. MLPA analysis). However, this can only detect a part of the changes (only deletions and duplications). Since most of the Fabry mutations known so far are missense mutations (exchange of a base pair in the DNA), this simple test cannot detect Fabry in most cases.
A complete analysis can only be carried out using “Next Generation Sequencing” (NGS for short). It must be ensured that intronic regions are also analysed, details of which we have already described here.
Unfortunately, there are information deficits here as well. We have a negative Fabry gene test which is only based on a simple MLPA analysis and therefore has almost no significance. In the information on the test used, the limitations are clearly explained, yet for the examining geneticist, Fabry was ruled out at that point. This is another piece of the puzzle as to why the diagnosis of rare diseases takes so long. Wrong tools are used by even professionals and so wrong diagnoses are made.
We are often contacted by patients with Fabry-related conditions who have intronic mutations in their genetics. Therefore, we would like to turn our and your attention back to intronic mutations:
Intronic mutations are an even broader topic. If you ask the Fabry experts, they usually explain that intronic mutations cannot do anything because there is no information in the introns. The answer is that simple and that wrong.
Briefly and simplified: on the one hand, there is also regulatory information in the introns that has an influence on enzyme production. On the other hand, certain sequences of the DNA sequence are used to determine between the introns and exons. If a new exon start is created by mutation in the intron, then the gene is read incorrectly (even if the “original” exons are all correct).
Unfortunately, most gene tests do not pay attention to intronic mutations at all, these areas are not analysed at all. But at the latest, if lyso-GB3-values or enzyme activity are abnormal, one has to search for the cause, which can then lie in the intron.
Various publications attempt to prove the apathogenicity of the controversial mutations. Some of them describe rather individual cases and are therefore not statistically reliable. Others refer to previous publications when making their statements. If you now look at the sources where the original statements with evidence come from, you will very often find two studies from 2003:
Yasuda: “Fabry disease: characterisation of alpha-galactosidase A double mutations and the D313Y plasma enzyme pseudodeficiency allele”.
Froissart: “Fabry disease: D313Y is an alpha-galactosidase A sequence variant that causes pseudodeficient activity in plasma”.
Both authors worked closely together, i.e. the studies are not independent! The studies show altered biochemical and physical properties of the modified enzyme. However, they then assume that these changes have no effect on the cellular level. But already in this study, disturbed processes in the cells are detected, which were later further investigated in studies on another controversial mutation. There it was shown that these changes lead to so-called ER stress (ER = endoplasmic reticulum). This ER stress is the cause of cell malfunction and even cell death. (see also Unfolded Protein Response)
I.e. the statements on apathogenicity are often not reliable or even wrong.
Therefore, most authors add that due to the small number of cases and various open questions, apathogenicity cannot necessarily be proven and further research is necessary.
Important Research that is made impossible by the deliberate filtering out of the controversial mutations in the gene laboratory.
Example:
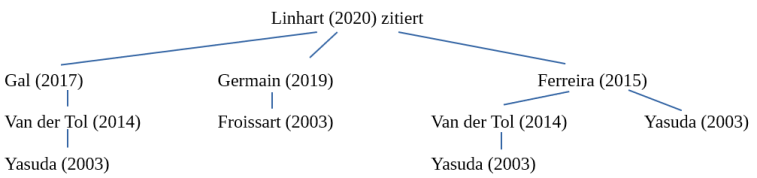
A publication from 2020 also refers to these two studies to prove apathogenicity.
In this publication (“An expert consensus document on the management of cardiovascular manifestations of Fabry disease”, Linhart et al. 2020) it was written: “As a cautionary example, the p.Asp313Tyr change results in a serum pseudodeficiency of AGAL-A activity and is not disease-causing. Similarly, a number of GLA variants previously thought to be disease-causing (e.g. p.Arg118Cys) have been shown to be of uncertain significance or likely benign. “(This is followed by a citation)
We have traced back the sources until we reached the original source:
In turn, the Varsome database cites Yasuda’s study as a source to prove pathogenicity.