Natascha and Berthold from MFSH were at FIN meetings in Amsterdam. FIN=Fabry International Network, an association of Fabry self-help groups from all over the world.
The presentation of the research work on “controversial variants” or D313Y was the highlight. The work could be presented to patients and scientists from all over the world.
IMPORTANT for all who have been genetically tested for Fabry disease in the last years! The laboratory findings may be incomplete and it could be that a variant is present but not reported.
Only pathogenic/disease causing variants are still reported in the findings!
The arbitrary classification of variants as benign/ benign by the laboratories means that they are no longer reported. The report only states:
NEGATIVE FINDING No clinically relevant variant was detected or No pathogenic variant found
It is not possible to determine an exact date for this procedure, as some laboratories were already practicing this before the GEKO decision. Here, the tests offered free of charge by the pharmaceutical industry stood out in a particularly negative way.
Background: The German Genetic Diagnostics Commission has decided that laboratories should only report disease-causing and probably disease-causing variants in their findings. Variants of unclear significance may be mentioned in the findings. Benign and probably benign variants should no longer be reported.
There are five classifications regarding the pathogenicity of mutations/variants:
In Germany, the controversy over the “controversial” variants of Fabry disease (a multi-organ disorder) has escalated further. Once again, some patients have had their therapy withdrawn. They had been in treatment for many years and felt a marked improvement in their symptoms. The focus was on devastating pain that could not be managed with standard pain therapy. Children also stopped treatment, although they clearly benefited from it. One child has been treated since the age of 4 and over a period of 7 years. Another child is now about to graduate from high school. Patients whose genetic defect was diagnosed in a stroke are also affected.
The first patients whose treatment was discontinued are already showing worsening symptoms. They are now in despair because they have experienced that the therapy has significantly improved their symptoms and because they now see no possibility of continuing to receive therapy. Parents are faced with the insurmountable task of explaining to their children why they are no longer receiving therapy.
Many of those affected can no longer imagine a life without the therapy and express this clearly. Some have already joined an euthanasia organization.
Patients who are still receiving therapy live with the constant fear that their therapy will also be terminated and have to helplessly watch others being taken off therapy or not receiving it at all.
The fact that these “controversial” variants do not make people ill is repeatedly claimed by various scientists, and there is also talk of a placebo effect. However, there are also other scientists who have proven a pathogenic effect of the variants. Because the experts are not in agreement, the discussion is now being carried out on the backs of the patients.
There is no question that the therapy helps, the drugs have a targeted effect only on Fabry, there is no known random effect in other diseases.
The claim that these “controversial” GLA gene variants do not cause Fabry is simply wrong! On the other hand, we can prove all our statements.
Yes, at least in a certain proportion of patients.
There is always talk of an enzyme deficiency that leads to deposits in the cells and then triggers the malfunctions. In many missense variants (i.e. an amino acid is altered somewhere in the DNA on the GLA gene) there is a residual activity of the enzyme. Nevertheless, the patients are often also severely affected. Here, another mechanism comes into play: ER stress or Unfolded Protein Response (UPR).
A brief explanation: Due to the variant, the enzyme is formed, but it is partly defective. Now a kind of “quality assurance” kicks in in the cell. The faulty enzyme is “repaired”. This is a normal process in the cells, since minor errors can happen again and again. However, due to the variant, the enzyme is permanently formed incorrectly and the error correction is overloaded. This is ER stress, which can lead to malfunctions of a cell or even cause cell death. Caperone therapy also “repairs” the wrong enzyme and relieves the cell. Here, enzyme replacement therapy would be less effective.
This mechanism has been demonstrated for some time, including for some of the controversial variants. But this explanation is not accepted by all scientists because it contradicts their own publications.
We patients are the ones who suffer; we are then prescribed no therapy or a less effective one.
In Fabry and many other diseases, a genetic test is used to determine whether there are changes in the DNA (genetic material) that can cause a disease.
For some time now, “next generation sequencing” has been available for this purpose, i.e. the actual sequence of information on a gene is determined. In the past, this was not possible and special tests were developed that were applied to very specific gene sections (e.g. MLPA analysis). However, this can only detect a part of the changes (only deletions and duplications). Since most of the Fabry mutations known so far are missense mutations (exchange of a base pair in the DNA), this simple test cannot detect Fabry in most cases.
A complete analysis can only be carried out using “Next Generation Sequencing” (NGS for short). It must be ensured that intronic regions are also analysed, details of which we have already described here.
Unfortunately, there are information deficits here as well. We have a negative Fabry gene test which is only based on a simple MLPA analysis and therefore has almost no significance. In the information on the test used, the limitations are clearly explained, yet for the examining geneticist, Fabry was ruled out at that point. This is another piece of the puzzle as to why the diagnosis of rare diseases takes so long. Wrong tools are used by even professionals and so wrong diagnoses are made.
Frequent misdiagnoses result in a Fabry diagnosis taking over 15 years on average. Many patients are never properly diagnosed. However, many of them could be helped causally. We have listed all known misdiagnoses here.
We are often contacted by patients with Fabry-related conditions who have intronic mutations in their genetics. Therefore, we would like to turn our and your attention back to intronic mutations:
Intronic mutations are an even broader topic. If you ask the Fabry experts, they usually explain that intronic mutations cannot do anything because there is no information in the introns. The answer is that simple and that wrong.
Briefly and simplified: on the one hand, there is also regulatory information in the introns that has an influence on enzyme production. On the other hand, certain sequences of the DNA sequence are used to determine between the introns and exons. If a new exon start is created by mutation in the intron, then the gene is read incorrectly (even if the “original” exons are all correct).
Unfortunately, most gene tests do not pay attention to intronic mutations at all, these areas are not analysed at all. But at the latest, if lyso-GB3-values or enzyme activity are abnormal, one has to search for the cause, which can then lie in the intron.
Various publications attempt to prove the apathogenicity of the controversial mutations. Some of them describe rather individual cases and are therefore not statistically reliable. Others refer to previous publications when making their statements. If you now look at the sources where the original statements with evidence come from, you will very often find two studies from 2003:
Yasuda: “Fabry disease: characterisation of alpha-galactosidase A double mutations and the D313Y plasma enzyme pseudodeficiency allele”.
Froissart: “Fabry disease: D313Y is an alpha-galactosidase A sequence variant that causes pseudodeficient activity in plasma”.
Both authors worked closely together, i.e. the studies are not independent! The studies show altered biochemical and physical properties of the modified enzyme. However, they then assume that these changes have no effect on the cellular level. But already in this study, disturbed processes in the cells are detected, which were later further investigated in studies on another controversial mutation. There it was shown that these changes lead to so-called ER stress (ER = endoplasmic reticulum). This ER stress is the cause of cell malfunction and even cell death. (see also Unfolded Protein Response)
I.e. the statements on apathogenicity are often not reliable or even wrong.
Therefore, most authors add that due to the small number of cases and various open questions, apathogenicity cannot necessarily be proven and further research is necessary.
Important Research that is made impossible by the deliberate filtering out of the controversial mutations in the gene laboratory.
Example:
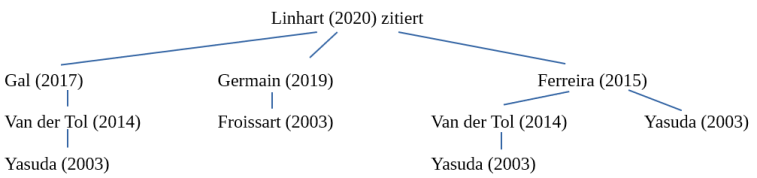
A publication from 2020 also refers to these two studies to prove apathogenicity.
In this publication (“An expert consensus document on the management of cardiovascular manifestations of Fabry disease”, Linhart et al. 2020) it was written: “As a cautionary example, the p.Asp313Tyr change results in a serum pseudodeficiency of AGAL-A activity and is not disease-causing. Similarly, a number of GLA variants previously thought to be disease-causing (e.g. p.Arg118Cys) have been shown to be of uncertain significance or likely benign. “(This is followed by a citation)
We have traced back the sources until we reached the original source:
In turn, the Varsome database cites Yasuda’s study as a source to prove pathogenicity.
There are five classifications regarding the pathogenicity of mutations/variants:
pathogenic – causing disease
likely pathogenic – probably causing disease
uncertain significance
likely benign
benign
In Germany the Genetic Diagnostics Commission has decided that laboratories should only report pathogenic and likely pathogenic variants in their findings. Variants of unclear significance can be mentioned in the findings. Benign and probably benign variants should no longer be reported.
Since there are a large number of benign variants in genetics, it seems perfectly understandable to filter them out.
But who determines whether a variant is pathogenic or not? And what about the variants where scientists do not agree (=unclear significance)? And who does the classification?
The classification can and must be done by each laboratory/doctor/centre itself. There are ACMG (American College of Medical Genetics) guidelines for this. However, these guidelines are under discussion, e.g. for Fabry itself. They also leave considerable room for interpretation. For example, the D313Y variant is classified by laboratories as “likely benign”. With other studies as a reference, this variant can also be classified as “likely pathogenic” (see e.g. Varsome database).
The literature situation is currently inconclusive; more recent work points to pathogenic factors. Nevertheless, some variants (such as the D313Y or A143T) have been reclassified as benign by some laboratories/centres and are now not even reported.
So, on the one hand, the stipulation of the Genetic Engineering Commission and the decision of doctors and laboratories is incomprehensible, because this actively keeps patients away from diagnosis and therapy. On the other hand, it also impairs research or even prevents it altogether.
We continue to fight for the controversial mutations, but the fight is severely and systematically hindered.